If you’ve recently been diagnosed with lipedema or suspect you have it, you may be wondering why the fat on your legs or arms feels different from “normal” fat.
As a physician specializing in lipedema, I often hear patients ask: What is the difference between lipedema fat and normal fat?
In this article, I’ll explain exactly how lipedema fat vs normal fat differ – from the way it’s distributed in the body to its microscopic structure – and why those differences matter.
My goal is to help you understand that lipedema fat isn’t ordinary fat at all, but a distinct medical condition – in other words give you the proof that Lipedema is not your fault.
What Is Lipedema? (A Brief Overview)
Lipedema is a chronic, genetically influenced fat tissue disorder that primarily affects women, causing a symmetrical buildup of fat in the legs and arms while sparing the hands and feet 1 2. Unlike typical fat distribution, lipedema fat accumulates disproportionately in the lower body and does not respond to diet or exercise.
Often triggered during hormonal changes like puberty or menopause1, it is frequently misdiagnosed as obesity, though it affects an estimated 11% of women1 and presents distinct structural and functional differences from normal fat.
Key Differences Between Lipedema Fat and Normal Fat
Lipedema fat has several important differences from the typical fat your body stores for energy.
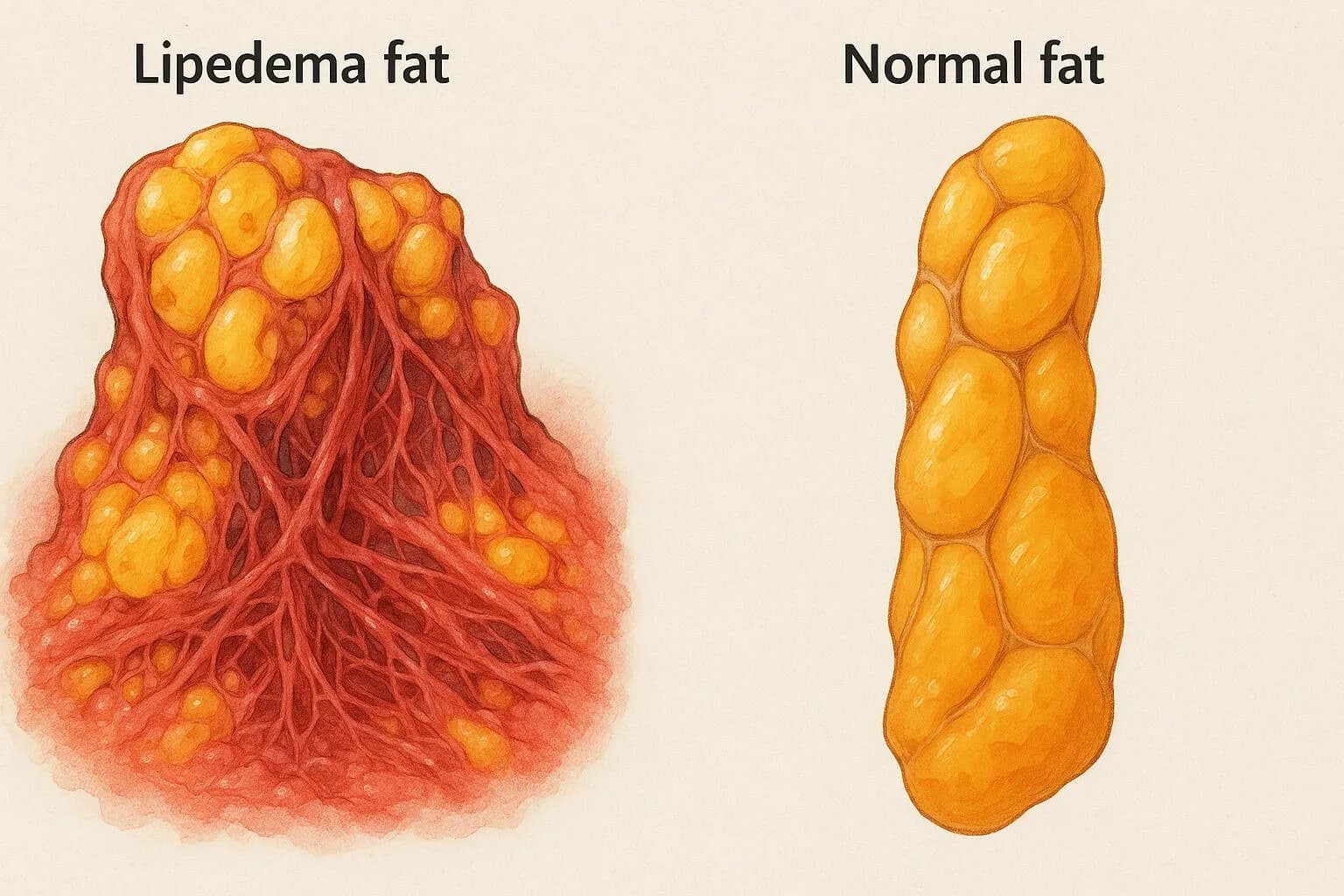
• Distribution and Appearance: Lipedema fat accumulates in a distinct pattern (legs and arms, bilateral and symmetrical, sparing feet/hands) unlike general obesity fat which is more diffusely distributed1. This leads to a characteristic “column-like” leg appearance or a cuff at the ankles, which is not seen in normal fat gain.
• Pain and Sensitivity: Unlike normal fat, lipedema fat can be painful to the touch and prone to easy bruising. Women with lipedema report tenderness in the affected areas and bruise easily due to fragile blood capillaries1. Ordinary fat tissue isn’t typically painful and isn't spontaneously bruised.
• Nodules and Fibrosis: Lipedema fat often feels firm or lumpy due to fibrotic nodules (pieces of hardened connective tissue within the fat). Under the skin, lipedema tissue shows fibrosis (scar-like tissue) and small nodules of fat, especially in later stages 3. Normal fat is usually soft and smooth without these fibrous lumps.
• Resistance to Weight Loss: Perhaps most frustrating, lipedema fat does not reduce easily with calorie restriction or exercise, whereas normal fat will usually shrink with weight loss efforts. Even bariatric surgery (weight-loss surgery) has limited impact on lipedema fat1 3. In other words, you can lose weight in other areas, but the lipedema-affected fat often stubbornly remains.
• Underlying Biological Differences: At a microscopic level, lipedema fat is inflamed and abnormal. The fat cells (adipocytes) in lipedema can be enlarged (hypertrophic) and increased in number (hyperplasia) 1. There is often more fluid between cells (edema) and impaired function of small blood vessels and lymphatics, leading to leakage and swelling. Normal fat tissue doesn’t show this level of chronic inflammation, fibrosis, or fluid retention. We’ll dive deeper into these scientific findings below.
Distinct Distribution: “Lipedema Fat Is Not Like Regular Fat”
One of the hallmark differences is where the fat accumulates.
In lipedema, the fat build-up is disproportionately in the lower body (and sometimes arms), while the feet and hands are unaffected. For example, a woman with lipedema might have very large legs and thighs, but normal-sized feet – leading to a bracelet or cuff-like fat ring just above the ankles. This is a classic sign of lipedema.
In contrast, common obesity-related fat tends to be distributed more evenly (including the feet if the legs are very swollen) or centered around the abdomen. Lipedema fat accumulation is typically bilaterally symmetrical – both legs (and both arms, if affected) enlarge at the same rate and to a similar extent1.
Furthermore, lipedema predominantly involves the subcutaneous fat (the fat just beneath the skin). It does not involve the deeper visceral fat around organs. Normal obesity can involve both subcutaneous fat and visceral fat (like belly fat around the organs). This is why someone with lipedema might have a relatively slim waist but very large legs. In short, the pattern of fat storage in lipedema is unique and diagnostic – it’s a disease of the limbs’ fat tissue rather than overall body fat.
This distinct distribution isn’t just a cosmetic issue – it reflects the underlying biology. The fact that lipedema fat spares the feet and hands is one clue that it’s not typical fat. It suggests an inherent tissue difference in the affected areas. Researchers note that lipedema fat tissue often expands in the legs and arms in ways that normal fat does not1.
So if you’ve noticed your lower body weight seems “stuck” no matter what you do, it’s not because you’re doing something wrong – it’s because lipedema fat behaves differently from normal fat.
Pain, Tenderness, and Bruising: “Why Does My Fat Hurt?”
Another major difference women with lipedema experience is that the fat hurts. Lipedema has been nicknamed a “painful fat disorder” because the affected fat can be tender or even painful when pressed, and legs often feel achy or heavy. Many patients also bruise easily in the lipedema areas without significant injury. Why does this happen?
In healthy normal fat tissue, there usually isn’t pain – fat is mostly storage tissue. But lipedema fat is abnormal and inflamed, and it’s interlaced with fragile blood vessels. Studies confirm that lipedema tissue is characterized by tenderness to touch (palpation) and easy bruising1.
Even a mild bump can cause a bruise on lipedema-affected legs because the capillaries (tiny blood vessels) in the tissue are weak and leaky. Chronic inflammation in the fat also irritates nerves, contributing to pain sensations.
Patients often describe the fat as feeling nodular or like “beans in a bag” when you press on the skin.
These nodules correspond to fibrotic tissue and trapped fluid (more on that shortly). The combination of swelling, poor circulation, and fibrous nodules means that lipedema-affected areas can be sore or sensitive, whereas normal fat tissue isn’t.
If your thighs are painful to touch or you have mysterious bruises on your legs, these are strong clues that the fat is lipedema, not just regular fat from weight gain1. This pain and bruising are key differences that highlight lipedema as a real medical condition of the fat – one that causes physical discomfort and is not just a cosmetic concern.
Under the Microscope: Structural Differences in Lipedema Fat
What really sets lipedema fat apart are the histological (microscopic) differences in the tissue. When scientists examine lipedema fat under a microscope and compare it to normal fat, the contrasts are striking. Here are some of the pathological changes found in lipedema fat that are not present in ordinary fat tissue:
• Enlarged Fat Cells (Hypertrophy): The individual fat cells in lipedema can grow exceptionally large. Research has shown that lipedema-affected fat cells (adipocytes) have a greater volume, especially as the disease progresses2. In other words, each fat cell in lipedema may hold more fat than a typical fat cell would, contributing to the disproportionate size of the limbs.
• More Fat Cells (Hyperplasia): In addition to being larger, there may be an increased number of fat cells. Lipedema fat tissue often shows signs of hyperproliferation of fat cells, meaning new fat cells are forming where they normally wouldn’t1. This is unusual because in adulthood, we don’t usually create many new fat cells – we just fill existing ones. Lipedema seems to be an exception, with fat tissue actively expanding via both cell growth and cell multiplication.
• Fibrosis (Scar Tissue) and Nodules: Healthy fat is soft and flexible, but lipedema fat becomes firmer due to fibrosis. Fibrosis is the accumulation of collagen and other connective tissue fibers, almost like internal scar tissue. Biopsies of lipedema fat show excess fibrous tissue woven among the fat cells, sometimes forming distinct nodules or lumps that you can feel 3. These fibrotic nodules make the fat feel firm or lumpy to the touch (hence the “beans or pearls” under the skin description). This fibrosis is a reaction to chronic inflammation and perhaps repeated trauma to fragile tissue. Importantly, this fibrosis is not seen in regular fat from simple obesity – it is a pathological change specific to lipedema’s disease process 3.
• Edema and Fluid Retention: The word “lipedema” has “edema” in it, which means swelling from fluid. Indeed, lipedema tissue holds more fluid between the cells. Microscopic analysis and imaging studies find excess interstitial fluid (lymphatic fluid) in lipedema fat1. This happens because the lymphatic system (which usually drains excess fluid from tissues) is not functioning well in these areas. The small lymphatic vessels in lipedema fat can be dilated and impaired, leading to sluggish lymph flow. Likewise, blood capillaries can be dilated and leaky. The end result is that fluid accumulates, causing swelling and that feeling of heaviness or puffiness in the limbs. Normal fat tissue does not have such lymphatic failure – it doesn’t harbor pockets of fluid in this way.
• Inflammation and Immune Cells: Lipedema fat is an inflamed fat. Under the microscope, we see many immune cells (like macrophages) infiltrating the tissue2. These cells release inflammatory signals that can further damage blood vessels and stimulate fibrosis. Interestingly, the type of inflammation in lipedema may differ from that in obesity. Obesity-related fat inflammation often involves pro-inflammatory immune cells that cause insulin resistance; lipedema, on the other hand, shows a pattern with more anti-inflammatory or pro-fibrotic immune responses (with many M2-polarized macrophages)2. In simpler terms, lipedema fat behaves like it’s chronically irritated or injured – the body responds by sending cells that cause swelling and scarring. This ongoing inflammation is why lipedema is progressive in nature. By contrast, normal fat (outside of extreme obesity) doesn’t usually have a bunch of immune cells hanging around – it’s not in a constant state of inflammation.
All these histological differences – bigger and more fat cells, scar tissue buildup, fluid accumulation, and inflammation – paint lipedema as a distinct pathology of the fat tissue. It’s not just fat sitting there; it’s diseased fat that’s actively malfunctioning.
These changes have been documented in clinical studies and distinguish lipedema from simple obesity or “normal” fat storage 1 2. Understanding these biological differences helps explain why lipedema fat behaves so differently (painful, stubborn, etc.) and reinforces that this is a real medical condition.
Why Lipedema Fat Doesn’t Budge with Diet and Exercise
Many women with lipedema find that no matter how healthily they eat or how much they exercise, the affected areas hardly slim down. This is not imagination – it’s a documented feature of lipedema. Lipedema fat is resistant to traditional weight-loss methods1. Patients can lose weight from the upper body or waist, but the legs and hips remain disproportionately large. Even bariatric surgery (which causes massive weight loss) often fails to significantly reduce the leg size in lipedema patients 3.
Why is lipedema fat so diet-resistant? The reasons tie back to the abnormalities we discussed above. The fibrosis in the tissue literally inhibits fat loss – studies suggest that fibrotic fat has impaired blood flow and metabolism, making it harder to break down fat for fuel 3.
Those enlarged, resistant fat cells are not only more numerous, but they also may not respond normally to the signals that trigger fat burning. Additionally, since lipedema fat often came on due to hormones and genetics rather than solely calorie surplus, simply cutting calories doesn’t fully reverse the process. It’s as if the fat in those areas has a “lock” on it.
By contrast, normal fat will usually shrink if you burn more calories than you consume. That fat is metabolically active and will be drawn upon for energy when you diet or exercise. Lipedema fat doesn’t get recruited in the same way, likely because of the combined factors of poor blood flow, lymphatic congestion, and cellular dysfunction in that tissue. As a result, women with lipedema often feel discouraged when weight loss efforts don’t affect their legs – but this is a key difference between lipedema and regular fat, and it’s not your fault or failure. In fact, recognizing this difference is important so that lipedema patients aren’t pushed into overly restrictive diets or blamed for not “trying hard enough.”
The science is clear: in lipedema, the fat’s behavior defies the usual rules of weight loss1.
What Causes Lipedema Fat to Be Different?
Lipedema isn’t caused by overeating, inactivity, or a lack of willpower. It’s a complex medical condition driven by factors like genetics, hormones, and connective tissue vulnerability.
While we’ve touched on how lipedema fat behaves differently from normal fat, understanding why it forms in the first place is equally important. I’ve written a comprehensive article that explores the root causes of lipedema in depth—from genetic inheritance patterns and hormonal triggers to vascular and connective tissue changes.
You can read it here: What Causes Lipedema?
In Summary: Lipedema Fat vs Normal Fat
To recap, lipedema fat is not normal fat. It is an inherited connective tissue disease that makes fat accumulate in a very particular way and renders that fat diseased and dysfunctional. Compared to normal fat, lipedema fat is:
- Differently Distributed: concentrated in legs/arms with feet and hands spared, leading to a disproportionate body shape1.
- Symptomatic: often painful, tender, and prone to bruising due to inflammation and fragile vessels1, whereas regular fat is not.
- Structurally Abnormal: filled with enlarged fat cells, excess fibrous tissue, and fluid deposits 2 3, making it firm and nodular rather than soft.
- Resistent to Diet and Exercise: resistant to calorie restriction and exercise, so it doesn’t diminish easily with weight loss efforts1, unlike typical fat which readily shrinks when you lose weight.
- Driven by Different Causes: triggered by genes and hormones, not by simple overeating. It often arises at life stages like puberty or menopause, highlighting that it’s a medical condition set in motion by factors outside your control1.
Understanding these differences can be empowering. It validates your experience if you’ve struggled with a “pear shape” that nothing seemed to fix. You are dealing with a real condition – a disorder of the fat tissue – not a failure of effort or willpower.
As a physician, I want to emphasize that lipedema is not your fault. It’s sometimes called “faultless fat” for this reason. The guilt or shame many women carry from having stubborn lower-body fat can be replaced with knowledge and, hopefully, effective medical management of the condition.
If any of these descriptions of lipedema fat resonate with you, you’re already taking an important step by learning about the condition. The next step is to get properly evaluated and seek out knowledgeable healthcare providers who understand lipedema.
If you haven’t yet, I strongly encourage you to take our 90-second Lipedema Quiz.
It’s a simple, evidence-based way to assess your risk and see if this condition might apply to you. Thousands of women have found clarity and a path forward by starting with that one step. Take the Lipedema Quiz here.
With hope and healing,
Dr. Jonie Girouard, M.D.
Lipedema Specialist | Founder, LipoedemaClinic.org
Dr. Jonie Girouard, M.D. is a global expert in Lipedema. She is the founder of the Lipedema Clinic, on a mission to educate and empower the millions of women still undiagnosed.
References:
- - Lipedema: Insights into Morphology, Pathophysiology, and Challenges https://pmc.ncbi.nlm.nih.gov/articles/PMC9775665/
- - Lipedema https://www.ncbi.nlm.nih.gov/books/NBK573066/
- - Standard of care for lipedema in the United States https://pmc.ncbi.nlm.nih.gov/articles/PMC8652358/#:~:text=match%20at%20L592%20Fibrosis%20of,Figure%203